Acute Abdomen causes, symptoms, types and treatment
Acute Abdomen refers to a sudden onset of severe abdominal pain that typically requires urgent medical evaluation and often surgical intervention. It is a medical emergency with a broad range of potential causes, including inflammatory, obstructive, vascular, and traumatic conditions.
Acute Abdomen
Acute abdomen is a critical condition that requires prompt assessment and intervention. Timely diagnosis and management can significantly reduce morbidity and mortality.
Acute abdomen: Any serious acute intra-abdominal condition attended by sudden, spontaneous severe pain in the abdomen that is less than 24 hours in duration. Acute surgical abdomen: Pain arising in a previously apparently healthy person that lasts more than six hours.
Causes of acute abdomen:
Acute Abdomen
Surgical Causes of Acute Abdomen
GIT Disorders:
- Non-specific abdominal pain (43%).
- Appendicitis (24%).
- Small & large bowel obstruction (5%).
- Perforated peptic ulcer (3%).
- Bowel perforation.
- Diverticulitis (2%).
- Gastritis and gastroenteritis.
Liver, Spleen & Biliary tract Disorders:
- Acute cholecystitis (9%).
- Acute cholangitis.
- Hepatic abscess.
- Ruptured hepatic tumour.
- Spontaneous rupture of the spleen.
- Splenic infarct.
Pancreatic Disorders: Acute pancreatitis (2%).
Urinary Tract Disorders:
- Renal colic (4%).
- Renal infarct.
Gynecological Disorders:
- Ruptured ectopic pregnancy.
- Twisted ovarian tumour.
- Ruptured ovarian follicle cyst.
- Pelvic inflammatory disease (PID).
Vascular Disorders:
- Ruptured aneurysm.
- Mesenteric vascular occlusion.
Peritoneal Disorders: Peritonitis or Intra-abdominal abscess.
Post-operative Causes:
- Bleeding or Abscess.
- Anastomotic leak.
- Bowel obstruction.
- Abdominal compartment syndrome.
Medical Causes of Acute Abdomen
Endocrine and Metabolic Disorders:
- Uremia.
- Diabetic crisis.
- Addisonian crisis.
- Acute intermittent porphyria.
- Hereditary Mediterranean fever.
Hematological Disorders: Sickle cell crisis.
Toxins and Drugs:
- Lead poisoning.
- Food poisoning.
Infections and Inflammatory Disorders:
- Henoch-Schonlein purpura.
- Systemic lupus erythematosis (SLE).
- Polyarthritis.
Tropical Diseases:
- Typhoid.
- Malaria.
- Tuberculous (TB) peritonitis.
- Amebiasis.
- Worm infestations.
Cardiac/Pulmonary Disorders:
- Pleurisy.
- Pneumonia.
- Cardiac disease. (e.g. myocardial infarction – MI).
Nervous System Disorders:
Disease of the spine affecting nerve roots.
Common Acute Abdominal Conditions in Infants and Children
- Acute appendicitis.
- Non-specific mesenteric adenitis.
- Intussusception.
- Intestinal volvulus.
- Meckel’s diverticulitis.
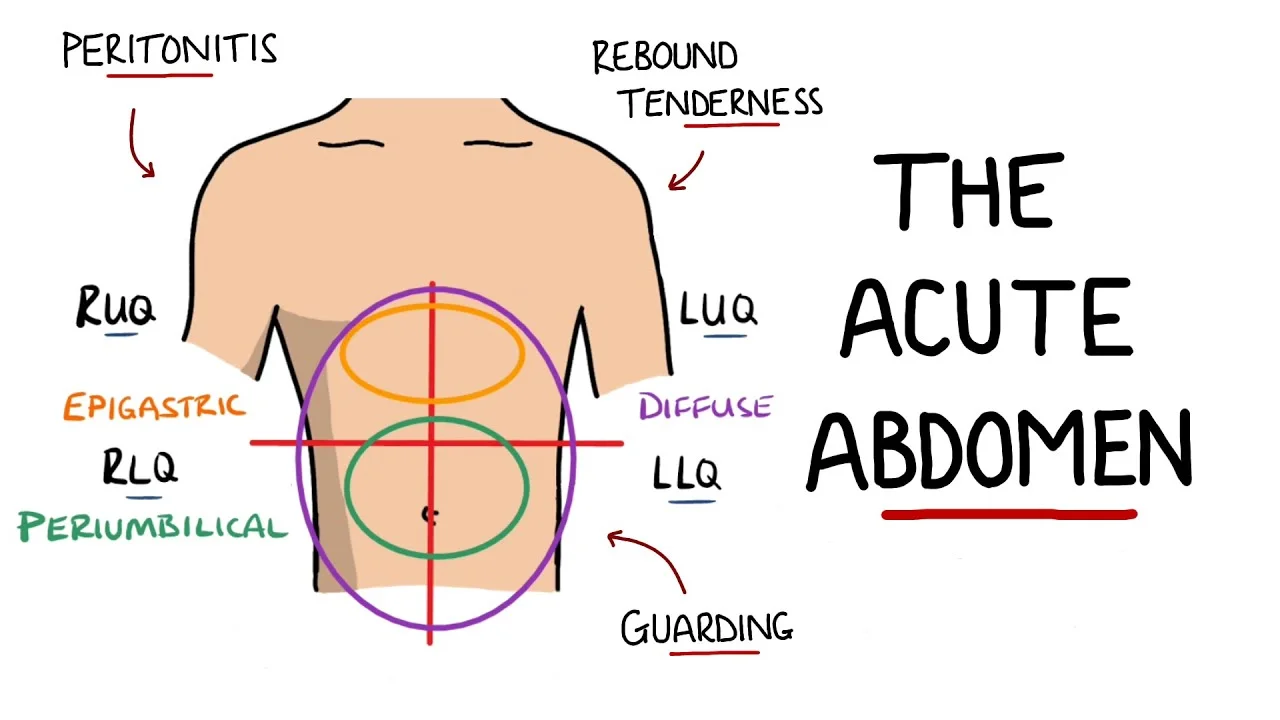
Common Causes of Pain According to Site:
1. diffuse (generalized) abdominal pain:
- GUT Perforation.
- Mesenteric ischemia.
- Abdominal Aortic Aneurysm (AAA).
- Acute pancreatitis.
- Diabetes mellitus (DM).
2. Localized abdominal pain:
Clinical diagnosis:-
History-Taking/Symptoms
1. Abdominal pain
location and character of pain.
- Visceral pain → dull, poorly localized (distension, inflammation, or ischemia).
- Parietal pain → sharper, better localized.
- Kidney/ureter → flank pain.
- Referral of pain (pain away from origin).
Onset
- Sudden (hemorrhage, perforation, or torsion).
- Gradual (inflammation).
2. GI symptoms
- Nausea, vomiting (bilious or bloody).
- Constipation is the rule in most acute abdomen (due to ileus or obstruction).
- Diarrhea (?? bloody).
- Both, nausea and diarrhea? Medical?
- Change in symptoms with eating?
3. Constitutional symptoms
- Fever Chills.
- Jaundice (passage of clay stools and dark urine denotes obstructive jaundice).
4. History-Taking
- Non-steroidal anti-inflammatory drug (NSAID) use (e.g. for duodenal ulcer).
- Drinking alcohol (pancreatitis).
- Prior surgeries (adhesions…).
- Hernia (obstruction, strangulation).
- Urine output (dehydration).
Clinical Examination
- General examination.
- Vital signs.
- Abdominal examination.
- Examination of hernial orifices.
- PR examination.
- Scrotal examination.
Investigations:
Laboratory Test
- Complete blood count (CBC): Leukocytosis or anemia.
- Electrolytes: Vomiting causes acidosis and dehydration.
- Amylase: Pancreatitis
- Renal function test
- Liver function tests (LFTs): Jaundice-hepatitis.
- Urine analysis: UTI – stones – hematuria.
- Stool analysis.
Imaging Studies
- Plain X-ray (supine and erect): Obstruction – free air – stones.
- Ultrasound: Cholecystitis – gynecological pathology – collection.
- CT scan: Diagnostic.
- CT angiography: Ischemia, bleeding, aortic aneurism.
treatment:
Primary Care
- Monitoring vital signs and pain assessment.
- Foley’s urinary catheter.
- Nothing orally (NPO) until surgical intervention is ruled out.
- Nasogastric (NG) tube with low continuous suction.
- IV fluids or nutritional support.
- Analgesia for pain.
Specific treatment (according to the diagnosed cause)
Decision to Operate (Indications of Surgery)
- Peritonitis: Tenderness, rebound tenderness, involuntary guarding.
- Severe/unrelieved pain
- Vitally unstable (hemorrhage or sepsis): Tachycardia, hypotensive, white count.
- Intestinal ischemia, including strangulation.
- Pneumo-peritoneum.
- Complete or high-grade obstruction.
Individual Causes of Acute Abdomen
Acute Appendicitis (the most common cause)
Clinical picture: This depends on the appendix’s site.
- Occur at any age.
- Pain starts in the umbilicus and then shifts to the right iliac fossa.
- Pain before vomiting.
investigations:
- Laboratory Test: High WBC counts with the shift to the left (leukocytosis).
- Imaging Studies: Ultrasound is used to exclude other pathologies, especially in females. e.g. Ectopic pregnancy or torsion ovarian cyst.
Treatment: Appendectomy.
Perforated Peptic Ulcer
clinical picture:
- Sudden onset.
- Commonly in the duodenum, (DU > GU with a ratio of 6:1.
- The ulcer may be acute or chronic.
- Board-like rigidity.
- History of precipitating factor e.g. NSAID.
investigation:
- Plain X-ray (KUB) shows air under the diaphragm (pneumo-peritoneum).
- Treatment: suturing and omental patch.
Acute Cholecystitis
clinical picture :
- Diffuse or colicky right hypochondrial pain with overlying tenderness and rigidity.
- examination: Difficult to feel the gall bladder (GB).
investigation: Ultrasound (US): cholecystitis – gall stones.
Treatment: cholecystectomy.
Acute Pancreatitis
clinical picture:
- History of precipitating factors e.g. alcohol intake and hyperlipidemia
- Severe epigastric pain and may be referred to the back.
- Profuse vomiting.
- The patient may be shocked.
investigation:
1. Laboratory Test:
- Serum amylase within 12 hours (elevated).
- Serum lipase (elevated) is more diagnostic.
2. Imaging Studies: US and CT scans are diagnostic.
Acute Diverticulitis
Clinical Picture:
- Rare before 40 years.
- Sigmoid is commonly affected.
investigation:
- Diagnosis relies on clinical presentation.
- CT scan is a diagnostic.
- Gastrograffin enema may be helpful.
Acute Intestinal Obstruction (refer to lecture on Intestinal Obstruction)
clinical picture:
- The four cardinal symptoms of bowel obstruction are pain, vomiting, absolute constipation, and distention.
- Rain is very severe and referred to as epigastrium, umbilical or hypogastrium.
- associated symptoms: fever, dehydration up to hypovolemic shock.
Symptoms according to site and cause of obstruction: In general the higher up the gut, the more severe symptoms.
small bowel obstruction:
causes: Hernia, adhesions, intussusception, cancer & volvulus.
1. Obstruction Proximal Small Intestine:
- Vomiting Very early, frequent and violent, green and bilious.
- Distension is minimal and not an early feature.
2. Obstruction Distal Small Intestine
- Pain is less severe than proximal small bowel obstruction.
- Vomiting and distension delayed.
Large Bowel Obstruction
- causes: volvulus, colon cancer, impacted fecal matter, etc.
- Distension is an early feature except in intussusception.
- Pain less acute, shock and vomiting late.
- Can be due to strangulation of the bowel where tenderness on applying pressure is positive.
Simple Bowel Obstruction
- Colicky abdominal pain.
- Abdominal distension.
- No fever.
- Absolute constipation + vomiting.
- Multiple air-fluid levels on plain X-ray.
diagnosis:
Strangulated/Bowel Obstruction
- Severe pain not relieved by NG tube.
- May be absent distention.
- Fever and tachycardia.
- Localized tenderness and guarding.
- Leukocytosis.
Vascular Acute Abdomen
1. Mesenteric Ischemia:
types:
- Acute mesenteric ischemia: Usually acute occlusion of the superior mesenteric artery (SMA) by a thrombus or an embolus.
- Chronic mesenteric ischemia: The patient is typically a smoker vasculopathy with severe atherosclerotic vessel disease.
clinical picture:
- The patient is over 50 years, with valvular or atherosclerotic heart disease.
- Arrhythmia or history of myocardial infarction (MI).
- Bleeding per rectum may be the early manifestation.
investigations: CT angiography is diagnostic.
2. Ruptured abdominal aortic aneurysm (AAA).
3. Ischemic colitis: Any inflammation, obstructive, or ischemic process can progress to perforation.
You can subscribe to Science Online on YouTube from this link: Science Online
You can download Science online application on Google Play from this link: Science online Apps on Google Play
Gastroesophageal Reflux Disease, Complications of GERD and Barrett’s oesophagus
Esophagus diseases, Dysphagia causes, Achalasia, and Symptomatic Diffuse Esophageal spasm
Pharynx function, anatomy, location, muscles, structure, and Esophagus parts
Tongue function, anatomy, and structure, Types of lingual papillae, and Types of cells in taste bud
Mouth Cavity divisions, anatomy, function, muscles, Contents of Soft palate and Hard palate
Temporal and infratemporal fossae contents, Muscles of mastication and Otic ganglion