Hyperthyroidism (thyrotoxicosis) causes, treatment and what is thyrotoxicosis Graves disease?
Hyperthyroidism is when the thyroid gland produces too much thyroid hormone, leading to an accelerated metabolism, The most common cause of hyperthyroidism is Graves’ disease, an autoimmune disorder, Other causes can include thyroid nodules or inflammation.
Hyperthyroidism
The prevalence of overt hyperthyroidism in elderly patients is 0.2 to 2%, which is similar to that in the general population. The prevalence of subclinical hyperthyroidism (suppression of TSH levels with normal T4 and T3 levels and usually without symptoms) is unknown.
Hyperthyroidism (thyrotoxicosis) causes
- The most common causes are Grave’s disease and multinodular toxic goiter.
- A solitary toxic adenoma is rare in elders.
- Adenomas are rare in the elderly, they autonomously produce and secrete excessive thyroid hormone even though TSH production is fully suppressed.
- lodine-induced hyperthyroidism, often from the use of amiodarone.
- Excessive ingestion of T4 ar T3 (either therapeutic or patient-initiated). (Factitious hyperthyroidism.).
Clinical picture
- Older patients have fewer symptoms and signs and a different complex of symptoms than younger patients.
- Only about 25% of elderly hyperthyroid patients present with typical symptoms and signs.
- Many of the age-related differences in symptoms are the result of the aging process and of concomitant disease that modifies the effects of excessive thyroid hormone.
- For example, the response to catecholamines decreases in elderly patients, possibly because of a decreased number or affinity of catecholamine receptors.
- Because catecholamines act synergistically with T3 to produce the typical symptoms and signs of hyperthyroidism, reduced responsiveness to catecholamines may explain some atypical symptoms.
- The classic triad in older patients is tachycardia, weight loss, and fatigue (or weakness or apathy), whereas in younger patients, it is tachycardia, goiter, and exophthalmos.
- Ocular signs are usually absent.
- Decreased appetite is common; increased appetite is the exception.
- Because the baseline heart rate decreases with age, heart rates > 90 beats/minute (rather than the standard of 100) must be interpreted as tachycardia in elderly hyperthyroid patients.
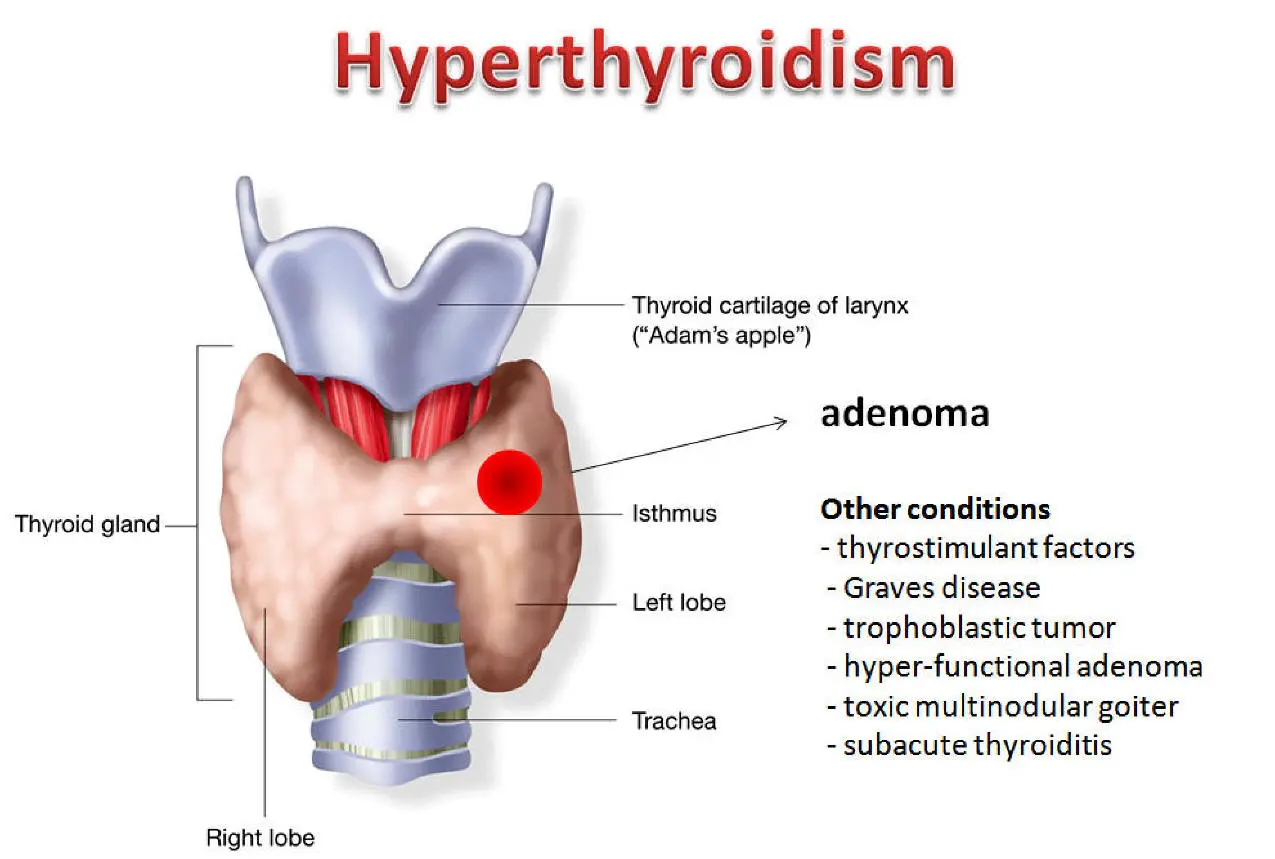
Hyperthyroidism
Regarding goiter
- The thyroid gland is normal in size or impalpable in about 40% of cases, enlarged and nodular in 35%, and enlarged and diffuse in 25%.
- Diarrhea is uncommon, whereas constipation is present in > 20% of elderly patients.
- Sweating is also far less common in elderly hyperthyroid patients.
- Nervousness and anxiety are less common.
- Tremor is almost as frequently seen as in younger patients.
- Hyperactive reflexes with quick recoil are far less common.
- Symptoms of heart failure and angina may dominate the clinical picture.
- Hyperthyroidism should be suspected in any patient with recent onset of cardiac disease.
- The most common complication in elderly patients is atrial fibrillation, which occurs in 27% of elderly hyperthyroid patients at presentation.
- Progression to heart failure and early death is increased if atrial fibrillation does not convert to normal sinus rhythm when euthyroidism is restored.
- Atrial fibrillation also carries a high risk of embolic stroke.
- Other features: Gastrointestinal (GI) symptoms may be confused with Gl malignancy.
- Other important complications are depression (called apathetic thyroidism). Myopathy and osteoporosis are common.
- A thyroid storm is a rare, life-threatening episode that may occur in the course of hyperthyroidism. It usually occurs when a stressful illness or event is superimposed on hyperthyroidism or occasionally when 131I therapy leads to massive leakage of thyroid hormones into the circulation.
- The symptoms and signs of hyperthyroidism are present, but the following also occur: fever, extreme tachycardia, nausea, vomiting, heart failure, and changes in mental status or consciousness. Serum T4 and T3 levels are no higher than in patients with usual degrees of hyperthyroidism. Thus, thyroid storm is a clinical diagnosis.
Diagnosis
- The best single test is the serum TSH measurement.
- A subnormal value suggests hyperthyroidism, and an undetectable value (< 0.01 mU/L) is almost pathognomonic.
- Serum FT3 & FT4, and thyroglobulin levels are on average lower in older patients with hyperthyroidism than in younger patients.
Treatment
The treatment of choice for most elderly patients with Graves’ disease or a single autonomous nodule is radioactive sodium iodide (131I).
It is preferred because it is easy to administer and it avoids any age-related postoperative complications of surgery.
Antithyroid drugs (eg, propylthiouracil, methimazole) are effective in the treatment of Graves’ disease if the patient’s adherence to the regimen is good. However, in patients with uninodular toxic goiter, antithyroid drugs are slow to work and rarely lead to permanent remission.
In multinodular toxic goiter, the response to 131I therapy is often delayed and incomplete. Because many doses of 131I may be needed, the patient remains hyperthyroid many months after the diagnosis. Thus, surgery may be preferred, at least for patients at low risk of postoperative complications. For patients at high risk, large and repeated doses of 131I should be given.
When hyperthyroidism is due to subacute thyroiditis, Hashimoto’s disease, or acute radiation damage, the only effective treatment is to give B-blockers and to closely observe the patient for complications.
Antithyroid drugs and 131I are not helpful because they do not decrease the uncontrolled output of hormones from damaged thyroid follicles. The usual treatment of iodine-induced hyperthyroidism is high doses of antithyroid drugs and a B-blocker.
Indications for Antithyroid drugs
- If 131I is refused by the patient.
- Before or after 131I is administered for rapid relief of symptoms of hyperthyroidism.
- Before surgical subtotal thyroidectomy.
- long-term therapy (1-2 years) to try to keep the patient in a euthyroid state until remission of the underlying disease is achieved.
Antithyroid drugs as primary therapy in elderly persons are administered in the same way as in younger persons. Propylthiouracil is given initially at 150 to 300 mg/day po in divided doses q 8 h. Maintenance dosing is 100 to 150 mg/day in divided doses q 8 to 12 h. The dosage is lowered sequentially based on symptoms and signs and serum hormone levels, which are monitored every 2 months. Serum TSH levels are useful. If the therapeutic response is inadequate, the dosage may be increased to 300 mg q 8 h.
Methimazole (Carbimazole) can be given as a single daily dose; the initial dose is 15 to 40 mg/day. The dose needs to be adjusted every 1 or 2 months, depending on the response. If the patient’s course is erratic with methimazole or propylthiouracil (eg, the patient slips quickly into hypothyroidism after small dose increases), the simplest solution is to add a small dose of levothyroxine sodium, usually 0.05 mg/day.
A pharmacologic dose of inorganic iodide (any dose > 6 mg/day) acts by inhibiting the release of thyroid hormone. The dose is generally effective for only 10 to 14 days. lodide is administered as Lugol’s solution (5% iodine and 10% potassium iodide), 2 to 6 drops tid (50 to 150 mg/day).
Thyroid storm
A thyroid storm is treated as an emergency. Treatment includes large doses of propylthiouracil (150 to 300 mg q 6 h) by nasogastric tube, if necessary; propranolol (1 mg by slow IV push q 5 min to decrease heart rate to between 90 and 110 beats/minute), and a glucocorticoid IV (hydrocortisone 100 mg immediately and 50 mg q 6 h thereafter).
Oral or IV sodium iodide (500 mg/day) can also be given, but ipodate sodium (3 mg in a single dose po or by nasogastric tube) is much more effective because it lowers the serum T3 level to normal within 24 hours.
You can subscribe to Science Online on YouTube from this link: Science Online
You can download Science Online application on Google Play from this link: Science Online Apps on Google Play
Histological structure of thyroid gland and Functions of Thyroid Hormones (T3 and T4)
Thyroid gland function, hormones, function, anatomy and Congenital anomalies
Posterior pituitary gland hormones & function, Control of ADH and Oxytocin hormone
Anterior pituitary gland function, hormones, location and Effects of Growth Hormone
Pituitary gland function, structure, location, hormones and anatomy
Endocrine system structure, function, disorders, Endocrine Glands and Hormone types